With causation settled, you write the plan that will guide treatment. The care plan captures goals, interventions, the expected frequency and duration of treatment, the return-to-work target, and any restrictions — the full shape of what you intend and why.
MTUSThe Medical Treatment Utilization Schedule (§9792), California's evidence-based treatment guidelines; for PTSD it makes TF-CBT the first-line intervention under §9792.24.2.CareHub Intelligence drafts an MTUS-aligned scaffold to start from — for Sofia's PTSD that means TF-CBT as the first-line modality under §9792.24.2 — and it cites the guideline behind each suggestion. The scaffold saves you the blank page; it does not set your goals. You set the goals, and you own them.
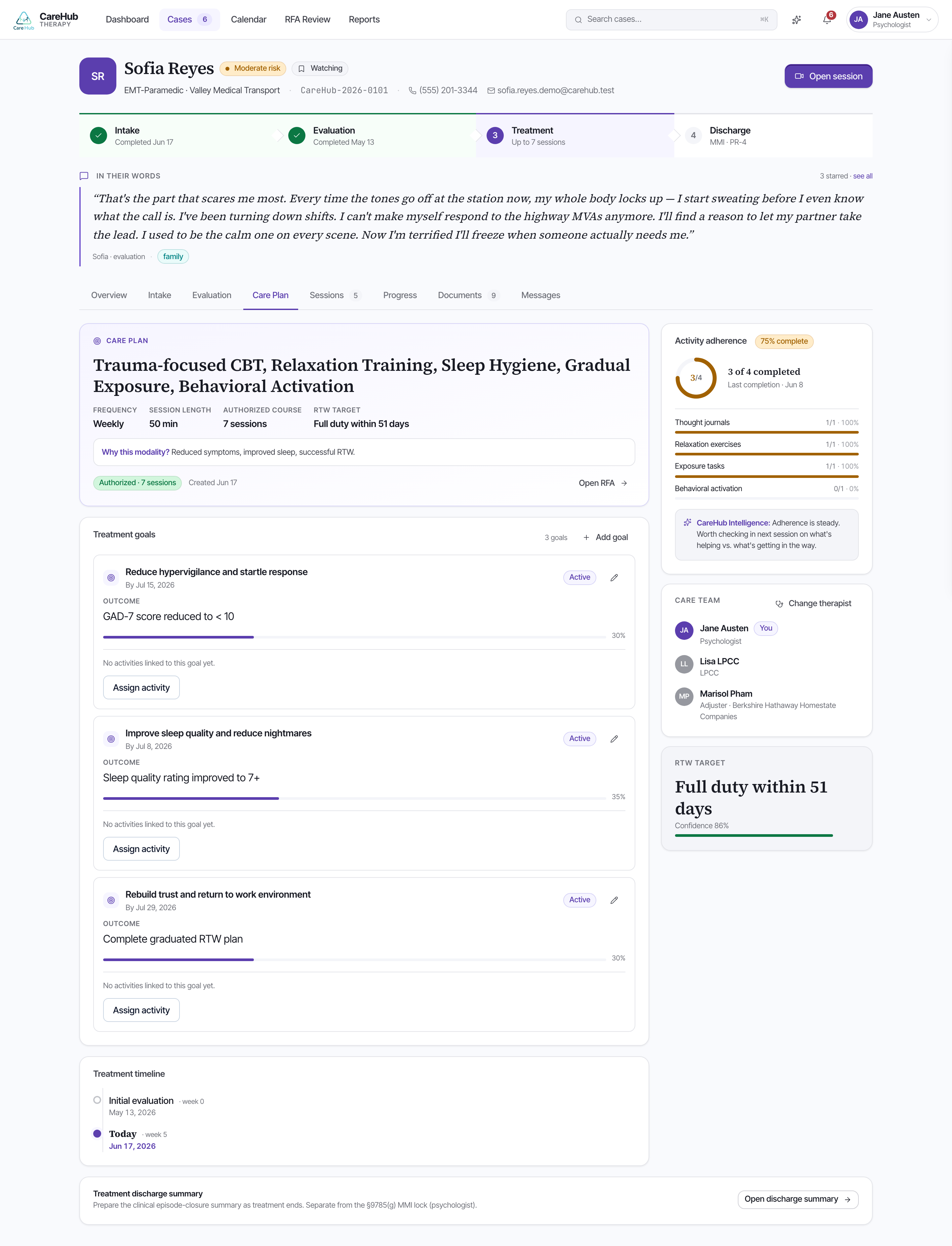
Goals must be measurable and tied to the screeners or GAF, because that is what makes progress provable later. "Reduce PHQ-9 from 17 toward remission" and "raise GAF from 52 toward pre-injury function" can be demonstrated; "feel better" cannot. The same goals feed her PR-2 progress reports and any RFA you co-sign.
This is the quiet hinge of the whole case. Every downstream document — the 45-day PR-2, the RFA that asks for more sessions, the discharge report — argues from progress against these goals. A goal anchored to a number you can re-measure is an argument that defends itself; a vague goal leaves your therapist with nothing to point to when the payer asks why treatment should continue.
So write the plan as the evidentiary spine it will become: measurable goals, the right MTUS-cited interventions, a realistic frequency and duration, and an RTW target you can move Sofia toward and show movement against.
Why does CareHub require care-plan goals to be tied to the screeners or GAF?