Treatment ends in one of two ways: the goals are met, or progress plateaus. The measurement you have been running tells you which. If about four consecutive sessions pass without measurable change on the screeners and check-ins, the plateau is your signal to reassess for maximum medical improvement rather than continuing on momentum. Either way, you mark treatment complete and turn to discharge.
discharge planthe patient-facing close-out of treatment — a plain-language summary, maintenance strategies, and crisis resources the member keeps after care ends.The discharge plan is written for the member, not the file. It summarizes the work you did together, lays out maintenance strategies to hold the gains — the grounding and coping skills from treatment, carried forward — and lists crisis resources so the member knows where to turn if symptoms return. This is the part of closure that belongs to you, the therapist who carried the treatment.
You prepare the discharge plan and mark treatment complete. The psychologist then declares maximum medical improvement and signs the PR-4 final report, which carries the §4663 apportionment of permanent disability. That apportionment, like the original causation determination, is psychologist-only — it is not yours to author. Discharge is a coordinated hand-back, not a solo close-out.
Frame the moment as a hand-back. You have run the treatment and built the measured record; you now pass a complete, well-documented case to the psychologist so the final report stands on solid evidence. The cleaner your notes, outcomes, and discharge plan, the easier the PR-4 is to defend.
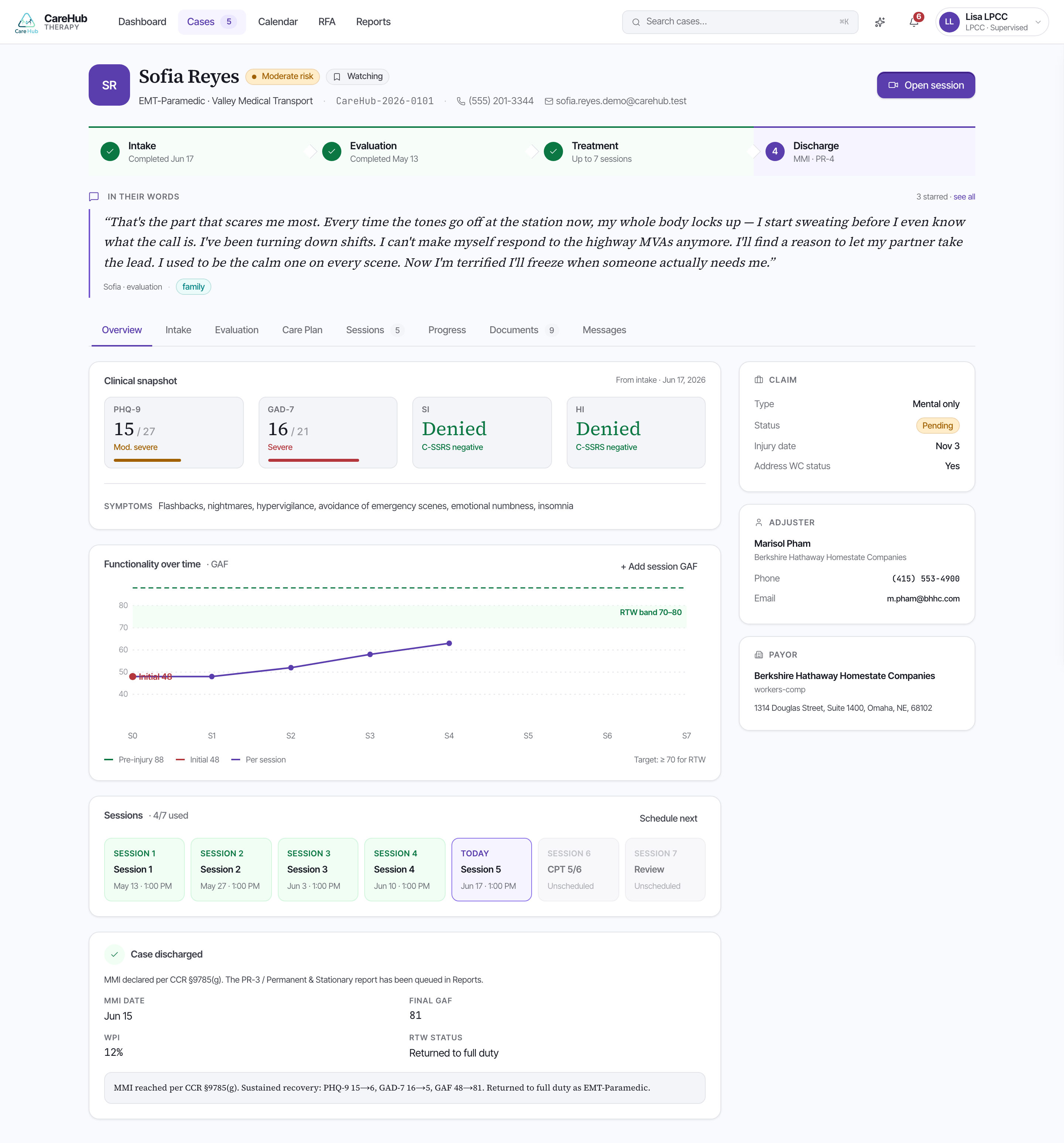
For Sofia, the case closes on a good note. Her PHQ-9 reaches 8 and her GAD-7 reaches 7 at MMI, her GAF has climbed from an initial 52 to a final 70, and she returns to modified duty. You prepare her discharge plan; the psychologist declares MMI and signs the PR-4.
At discharge, what does the LPCC do and what does the psychologist do?