Measurement-based care is the engine of a defensible Workers' Comp case. A case that improves but cannot prove it will struggle at utilization review; a case with a clear measured trajectory carries its own argument. Your job is to keep that measurement running.
Re-administer the PHQ-9 (0–27, depression) and GAD-7 (0–21, anxiety) at baseline and about every four sessions. Capture the GAF each session — four timepoints accrue across the case. Between visits, lightweight check-ins on mood, sleep, and anxiety, together with activity adherence, fill the gaps the formal screeners leave. The Outcomes view trends all of it on one surface so the trajectory is visible at a glance.
reliable changea movement of at least 5 points on the PHQ-9 or GAD-7 — large enough to represent genuine clinical change rather than measurement noise.This is a closed loop: assign activities, watch the member adhere, measure with the screeners and check-ins, and adjust the plan to what the data shows. That loop is exactly what your PR-2s and RFAs cite as proof of progress. The numbers are not paperwork; they are the case.
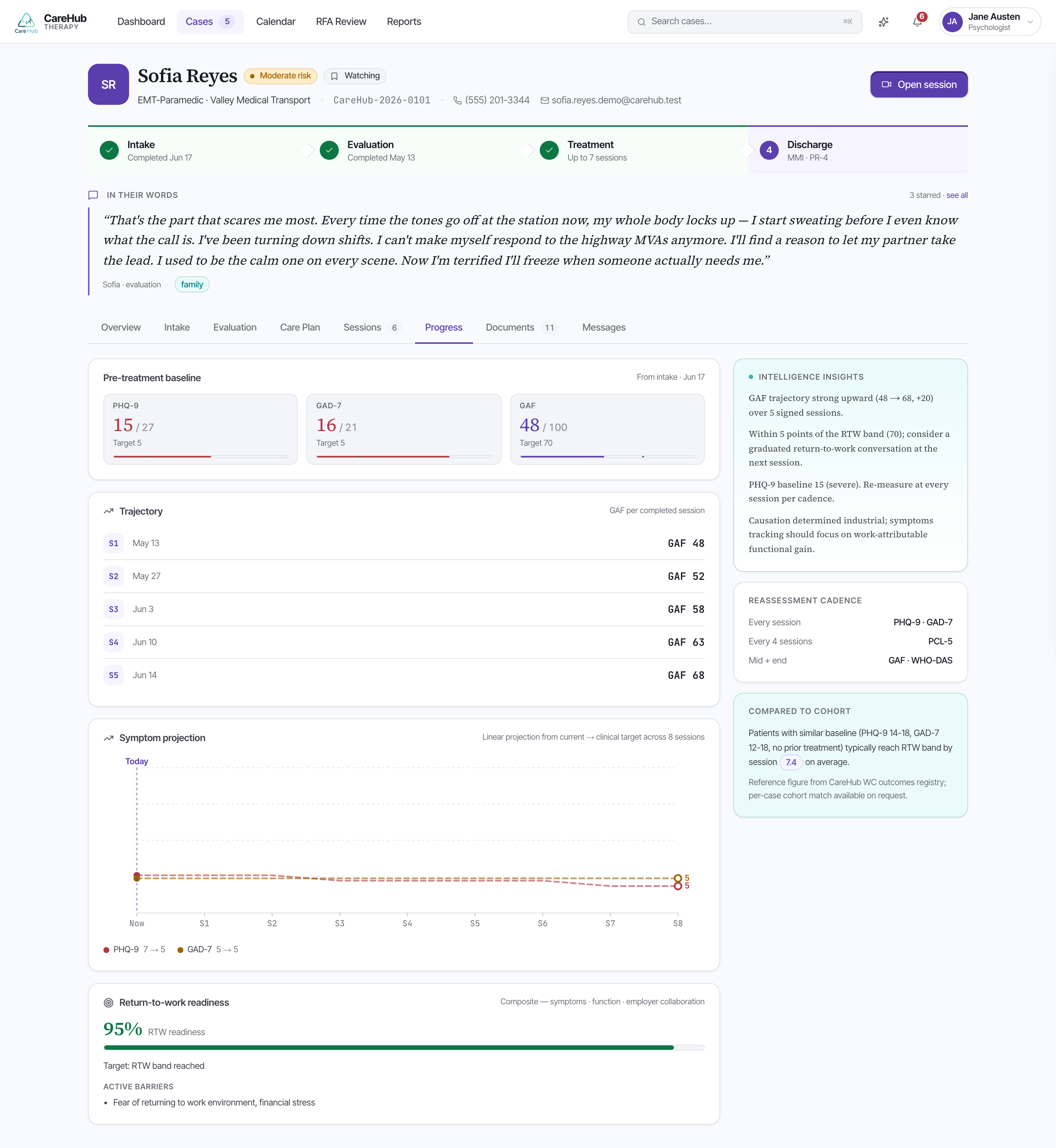
On the teaching case, Sofia's screeners move the right way. By session 6 her PHQ-9 has gone 17 → 12 and her GAD-7 16 → 11 — each a 5-point drop, so both meet the reliable-change threshold. That is the evidence that the plan is working and that more sessions are warranted.
PHQ-9 Item 9 screens for thoughts of self-harm. A positive response triggers a C-SSRS and your safety protocol — this takes priority over the rest of the measurement workflow. Respond to the risk first; the scores are secondary to the person.
By session 6 Sofia's screeners read PHQ-9 17 to 12 and GAD-7 16 to 11. How do you read this in the Outcomes view?