As the licensed therapist on a case, you step in after the evaluation is finished. The psychologist has examined the worker, reached a diagnosis, rendered the causation determination, and written the care plan. You inherit all three. Your work is the ongoing arc: running treatment, documenting sessions, and keeping the case moving through its reporting and authorization cycles.
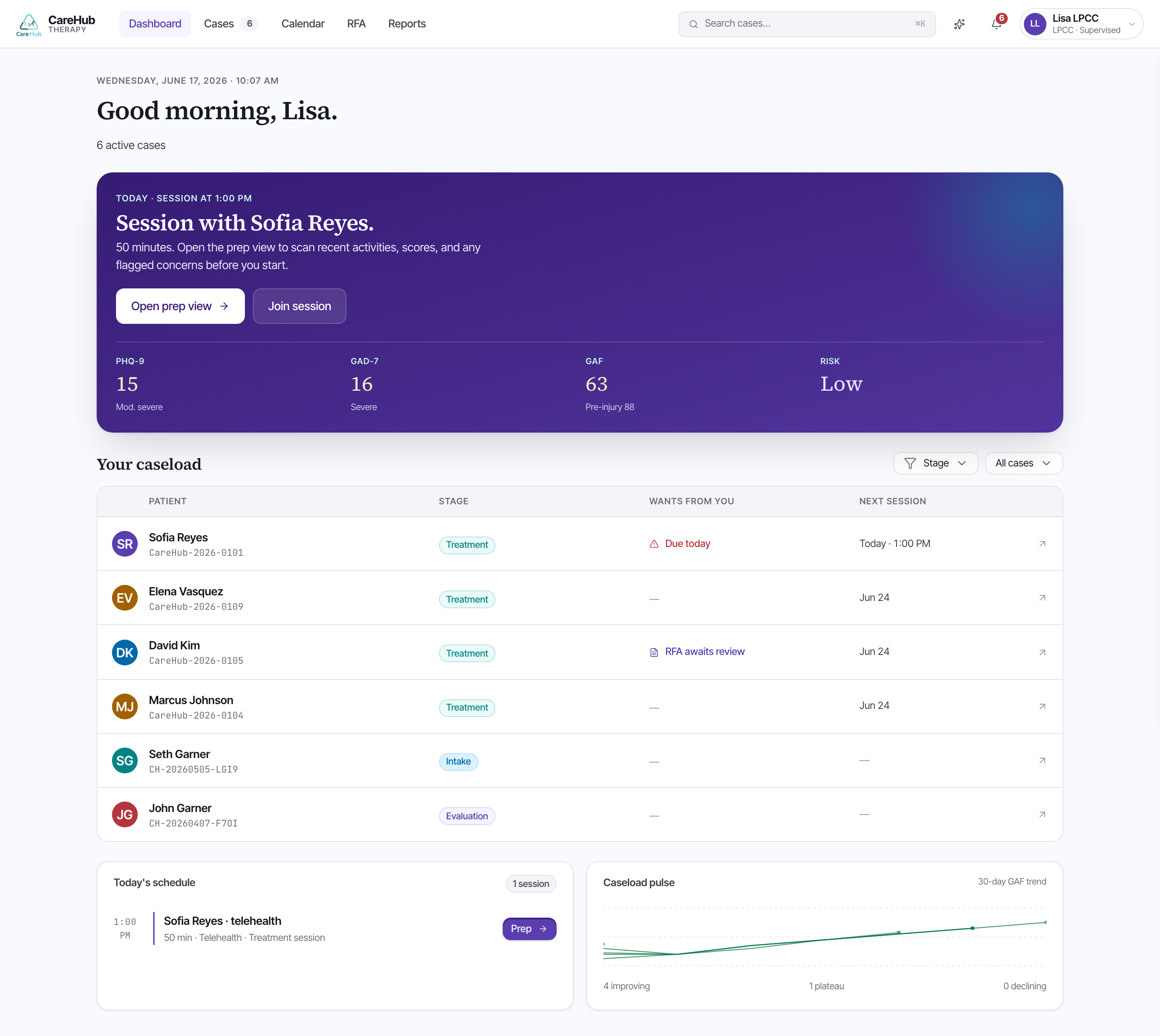
Your dashboard is built around that work. Rather than a static roster, it organizes the caseload by what needs you right now — newly assigned cases waiting to be picked up, sessions to run, reports to draft, and authorization responses that have come back. The queue is the point: open the case at the top of the column that is asking for action.
LPCCa Licensed Professional Clinical Counselor — the therapist who delivers ongoing treatment under the psychologist's care plan and causation determination.When you open a case, the diagnosis, the causation split, and the care plan are already on the chart. You read them; you do not author them. On the teaching case, Sofia Reyes — a paramedic who witnessed a fatal multi-vehicle collision — arrives with a PTSD diagnosis (F43.10), a causation determination of industrial, and a TF-CBT care plan with seven sessions authorized. That is your starting line.
You run treatment, document sessions, and draft the PR-2 progress reports and RFAs. The psychologist owns the evaluation, the causation determination, the evaluation signature, and the co-signature on every RFA. You draft; they co-sign. You never author the causation opinion at all — that boundary holds through the whole case.
Knowing which seat you are in keeps the case clean. When an adjuster questions causation, the answer comes from the psychologist's signed opinion, not from you. When the case needs proof that treatment is working, that evidence is entirely yours to build.
A case lands in your queue. Which of these is the LPCC's job?